

What is congenital adrenal hyperplasia?
Congenital adrenal hyperplasia (CAH) is an inherited hormone disorder that affects children and adults worldwide. The most common form of CAH is estimated to occur in 1 in 15,000 newborns and is the type discussed here. In certain ethnic populations, like the Yup’ik indigenous peoples of Alaska and in individuals of Saudi Arabian ancestry, CAH is more frequent.
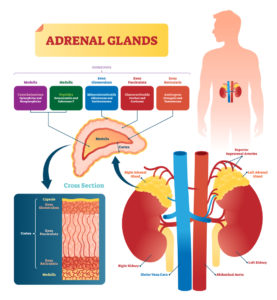
The adrenal glands make hormones in the body. An enzyme found in the adrenal glands, called 21-hydroxylase (21-OHD), is responsible for making cortisol and aldosterone. These hormones have many functions, including maintaining healthy blood pressure and salt/electrolyte balance. In 90% of people with CAH, 21-OHD does not work properly. This blocks the usual metabolic pathway, leading to low cortisol and aldosterone levels and the symptoms of what is called 21-OHD CAH.
What are the symptoms of 21-OH CAH?
21-OHD CAH is divided into groups. The signs and symptoms of 21-OHD CAH vary by type:
- Simple virilizing type (~25% of people): This type can be identified as early as during a pregnancy. It can cause babies that are biologically female to have male-appearing external genitalia (“virilization”), although they usually have a uterus and fallopian tubes. Virilization is not easy to notice, if at all, in babies that are biologically male. Hormone treatment can help with growth and puberty, in addition to maintaining fertility.
- Salt-wasting type (~75% of people): In addition to the above symptoms, these babies have poor feeding, weight loss, severe dehydration, and usually develop an adrenal “crisis” by four weeks of age. This life-threatening issue needs urgent medical treatment. Babies that are biologically male are particularly vulnerable to this crisis — the effects of virilization are not noticeable in them and their diagnosis may go unnoticed.
In areas where it is available, babies are screened for 21-OH CAH shortly after birth as part of a newborn screening program.
How is 21-OH CAH inherited?
21-OH CAH follows an autosomal recessive inheritance pattern. It is associated with having two pathogenic variants, or mutations, in the CYP21A2 gene. Parents of someone with 21-OH CAH usually carry one CYP21A2 mutation and are called “carriers.” Carriers typically do not have obvious symptoms. There may be no one with CAH in the family, so someone may not know they are a CAH carrier. This is important when considering a pregnancy, particularly for people that come from an ancestry group where CAH is more common.
How can someone find out if they are a 21-OH CAH carrier?
Genetic testing for 21-OH CAH is available. Some tests, such as expanded carrier screening, are available even without a family history of a particular condition. Expanded carrier screening may not be covered by health insurance, so it is important to talk to your healthcare provider and identify any out-of-pocket costs before having testing done.
How is CAH treated?
Different treatments are available for CAH:
- Hormone medication, which may be given during a pregnancy known to have CAH
- Specialized diet to increase salt intake
- Surgery
People with CAH can benefit from coordinated care that different medical specialists provide.
Is preimplantation genetic testing available for 21-OH CAH?
Yes, with one of the earliest reported cases published in 1999. The option of PGT provides a different route to conception that may help reduce anxiety for families at risk for 21-OH CAH, particularly when there is uncertainty about the potential success or availability of treatments. Many factors play a role in whether or not parents decide to pursue PGT. Meeting with a genetic counselor before becoming pregnant is the best next step to explore the risk to have a child with CAH and discuss the option of PGT.
For more information and resources about congenital adrenal hyperplasia, please visit the CARES Foundation website.

Deepti is an independent consultant for Sharing Healthy Genes. She is a highly skilled writer and editor with medical communications and marketing experience, which blends with her 20+ years of clinical acumen as a certified genetic counselor in the U.S. and Canada. Deepti has an active consulting business and is an engaged member of the National Society of Genetic Counselors, most recently serving as a 2018-2020 Director at Large. In her downtime, you’ll find Deepti poring over cookbooks, facing down superhero quizzes from her sons, or writing about her family’s foodie gene on her blog.